By the early 1990s, the Goodfellow Unit had developed a reputation as a leader in providing continuing medical education for GPs and other primary health care workers. It was in a strong position to compete for Regional Service Contracts that became available with the establishment of four Regional Health Authorities (RHA) in 1993. The National Government had established the RHAs as part of their ‘radical reform’ of the country’s health sector, and each RHA became responsible for funding health care in their respective areas.[1]
Staff from the Goodfellow Unit started to apply for funding that was available for primary health care education. As Jocelyn Tracey, the then Assistant Director of the Goodfellow Unit recalled, ‘it was quite an entrepreneurial time!’
The Immunisation Advisory Centre est. 1994
In 1994, the Goodfellow Unit received a contract to provide immunisation coordination services for the Auckland and Northland regions. The contract arose in response to national concerns about the low childhood immunisation rates, as revealed in the New Zealand Communicable Disease Centre childhood immunisation coverage survey 1991/2.[2]
Under the direction of the nursing coordinator Elaine Boyd, the Goodfellow Unit developed the Northern Region Immunisation Support Service or NRISS. From 1995, NRISS started to work with the Well Women’s Nursing Service – now called the Well Women and Family Trust – to offer vaccination-training programmes in Auckland.
In 1997, Elaine Boyd and other Goodfellow staff members – who ‘very much wanted to pull general practice into the immunisation arena’ – appointed Dr Nikki Turner as the regional immunisation coordinator for the NRISS network within the Goodfellow Unit.[3] Nikki had completed her medical training at the University of Auckland in the late-1980s. She then spent several years in England where she completed her postgraduate training in paediatrics. Nikki started to attend the Goodfellow Unit’s evening and weekend courses shortly after she returned to New Zealand. She reflected on these sessions as ‘well run and well attended’ and as offering her with opportunities to establish a community with other general practitioners.

Nikki had gained considerable experience working with community health before she joined the Goodfellow Unit. She had co-established Wai Health at Te Waipareira Trust with Dr Sue Crengle, and a general practice clinic with another colleague in the Auckland City Mission.
She joined the Goodfellow Unit as the immunisation coordinator at a time when:
People weren’t getting their kids vaccines at all, or they were getting them late. And a lot of it was just simple systems problems: people didn’t get reminded, they didn’t get recalls, the general practice systems weren’t set up to help people easily get their kids vaccinated … In the early days, we did a lot around how the general practice operates to make it easy for people to vaccinate their babies.[4]
With support from the University of Auckland and a contract from the Northern Regional Health Board to develop a regional communications strategy, Dr Turner and colleagues launched The Immunisation Advisory Centre (IMAC) in 1997. She developed the brand and established a national phone line to communicate immunisation advice more effectively to health professionals and other members of the public.[5]
Several clinics across Auckland and Northland had already launched interventions into New Zealand’s low immunisation rates. Nikki’s role involved ‘becom[ing] the glue for all these different organisations’ and developing a communication strategy. They aimed to establish a universal base ‘so every kid was known and every kid belonged in a general practice, and then the general practice have a trusting relationship with the family where they can communicate with them and have adequate tools to make that communication happen easily’.
These tools included the development of the National Immunisation Register, a computerised information system that contained the immunisation details of each child across New Zealand, in which IMAC was involved. In addition to ensuring GPs recorded each child’s immunisation history, IMAC staff also aimed to help GPs and practice nurses to develop confidence in their knowledge of immunisation and in their skills in providing vaccinations. Nikki explained:
When your system works well and your providers are confident and knowledgeable and they have good relationships with families, then vaccine hesitancy is not such a big deal, it’s just a small percentage. And I think when your system doesn’t work well, providers aren’t confident, they don’t communicate well, and parents get more anxious.


Elaine Boyd returned to work with IMAC and addressed queries on the phone line, 0800 Immune.
While parents had to make the ‘active decision’ to immunise their children in the late-1990s, Nikki explains that ‘with all the systems in place now, people would have to make an active decision to choose not to immunise’. IMAC achieved its aim to ‘normalise childhood immunisation as “This is what you do. This is normal to the community”’.[6]
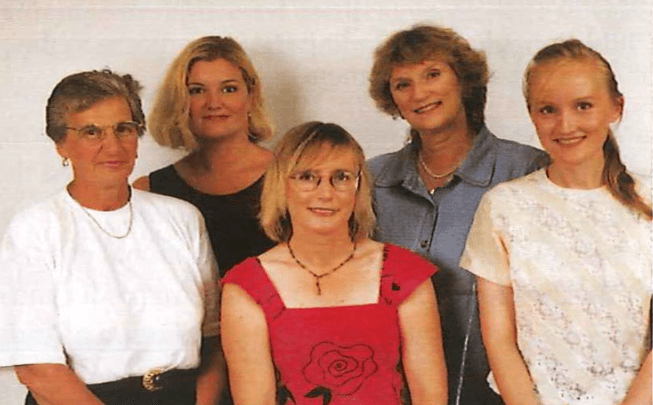
IMAC Staff (L-R) Kathleen Dewson – Secretary, Jane Cunningham – Project Nurse Coordinator, Dr Nikki Turner – Medical Advisor and Director, Elaine Boyd – Nurse Co-ordinator, Dr Phillipa Clark – Paediatrician. Image supplied by Nikki Turner
The Immunisation Advisory Centre is now a nationwide organisation that provides health professionals and the New Zealand public with evidence-based advice about the risks and benefits of immunisation. Nikki attributes their ability to develop IMAC in the late-1990s to both the supportive environment of the Goodfellow Unit which ‘had the ability to do new and novel stuff which doesn’t always happen’, and the Regional Health Authorities that ‘were willing to try innovative new approaches’.[7]
Tobacco, Alcohol and Other Drugs, 1995 – 2005
The Tobacco, Alcohol and Other Drugs brief intervention training project, or TADS, arose in response to international concerns about the impact of alcohol on communities. In 1980, the World Health Organization Expert Committee on Problems Related to Alcohol Consumption called for appropriate systems to identify people at risk of alcohol abuse, and to instigate appropriate interventions.[8] Consequently, in 1982, the WHO initiated their Collaborative Project on Identification and Treatment of Persons with Harmful Alcohol Consumption. TADS formed part of New Zealand’s response to instigate early and brief intervention for people at risk of alcohol or other drug abuse.
In 1995, the Goodfellow Unit won a funding bid from the Regional Health Authorities to run the Tobacco Alcohol and Other Drugs brief intervention training project. The funding bid was a collaborative effort between Drs Phil Barham and Jocelyn Tracey from the Goodfellow Unit, Ross McCormick who was then an Associate Professor in the Department of General Practice, and Peter Adams, clinical psychologist and part-time lecturer at the University of Auckland.
The project aimed to address the identified barriers to GPs’ abilities to launch early and brief intervention into patients’ struggles with alcohol and other substances. These included the lack of organisation and supportive government policies, insufficient training, lack of funding, GPs’ lack of time, and intervention being deemed ‘too difficult’.[9] Funding from the RHA enabled the Goodfellow Unit to employ staff to train GPs, practice nurses, and other health care providers to recognise drug and alcohol abuse and to implement early and brief intervention. This involved delivering short courses to primary health care workers on smoking cessation, recognising the signs of alcohol and other drug abuse, and on appropriate forms of intervention, among other topics.

In December 1995, Phil Barham and Jocelyn Tracey appointed Rose Lightfoot, a registered nurse with twelve years of experience teaching nursing at Te Wānanga o Whangarei and then at Unitec in Auckland, as the project manager. Rose remembered the interview in 1995 as ‘the very first interview that I’ve ever had that I really enjoyed’. She was ‘delighted’ to be was offered the position.[10]
Rose explained that the Tobacco, Alcohol and Other Drugs project aimed to establish ‘a really well built programme of introducing brief and early intervention and the options for getting people to address their issues of addiction with any of these substances’.[11] Developing such a programme involved engaging with an advisory board, which included Peter Watson as the adolescent representative, Moira Douthet as the Pacific advisor and Pam Armstrong from Kia Ora Ngatiwai, an iwi health provider in Northland to develop appropriate teaching. Rose explained that these advisors ‘contributed from their own areas of expertise to the general issue of how to manage drug and alcohol people with these special population groups’.[12]
The courses proved to be popular among general practitioners. Across the 1990s, the TADS project reached nearly 500 participants per year. By 2001, this number had tripled to nearly 1500 participants per year after it was heavily marketed to primary healthcare nurses.[13] Rose attributed the high demand of the courses to the difficulty of managing alcohol and other substances, especially considering the limited GP consultation time.
Considering the emotional intensity of the topics they covered, the course facilitators carefully planned the sessions to provide ‘light hearted but really pointed education’. They aimed to ‘improve the skill base of general practitioners and make it more effective and more enjoyable for them in the work that they were doing, so it was very much hands on with lots of interactions’. Rose cited the teaching quality of Goodfellow Unit staff as key factors in the success of the programme. She described her colleagues, namely advisor Jocelyn Tracey and course facilitators Bruce Adlam and Mark Shaw, as ‘all really innovative teachers. We tried to make all the classes and the options that we ran really attractive so we called them by crazy names. It was a lot of fun and we wanted people to enjoy coming and to get something that they could take away and put into place the next day’.[14]
While the courses primarily focused on GPs based in Auckland, they also took the courses on a ‘travelling roadshow’ to Dargaville, Hokianga, Kaitaia, and Whangarei, and hired local actors for the role-play scenarios. They engaged with wider community groups so ‘that there were people with expertise out there that each of the professional groups could draw on if they needed to’.
Rose left the Goodfellow Unit in December 1998, and encouraged Barbara Docherty, a registered nurse, to apply for her position. Barbara had completed her nurse training at the Mater Misericordiae Hospital in 1965. She had worked as a nurse practitioner in Auckland, had published a guidebook on nursing in general practice, and had contributed columns to GP Weekly and the NZ Doctor, among other avenues. She joined TADS in late 1998 to implement the third and fourth stages of the WHO Collaborative Project, which involved consulting with stakeholders and developing TADS into a national programme.
Barbara Docherty on taking over Rose Lightfoot
In 2000, the project extended to focus on reducing the ‘harmful effects of unhealthy behaviour’. In addition to tobacco, alcohol and other drugs, TADS also focused on gambling, physical inactivity, and mental health risks, among others.[15] During an interview for the Alcohol Advisory Council of New Zealand in 2001, Barbara described their emphasis on ‘supporting and motivating patients to recognise and actively change present or potential problems related to substance use and abuse’. [16]
Barbara described the Goodfellow Unit as a ‘Terrific foundation for something that was very new and needed to be recognised as a necessary type of training for GPs and other primary health care professionals’. They ‘had to reach out to the community and ask them what they wanted and bring it back and try and make it work. Rather than setting up an academic-type training and saying, “You need us”, it was the other way around. “We need the community, we need you, how do we make this work?”’[17]
Funding ended in 2005, by which time Goodfellow staff had trained thousands of health professionals in detecting patients’ misuse of alcohol and other substances and establishing appropriate forms of intervention.[18] Since 2005, Barbara had continued the work in a private capacity, independent from the Goodfellow Unit. She is the current director of TADS, now known as the Training and Development Services.
Quality Assurance Unit, c. 1990s
In the early-1990s, the Goodfellow Unit also became responsible for regulating the quality of general practices by hosting the Royal College Quality Assurance Unit.
In 1992, Drs Phil Barham and Jocelyn Tracey appointed Dr John Wellingham as the Quality Unit Director. Like most other Goodfellow Unit staff at that time, he was on a part-time contract
alongside his clinical work. Dr Wellingham had completed his medical training at St Bartholomew’s Hospital in London. He moved to Wellington in 1976 and worked alongside Professor Tom O’Donnell for one year, and then gained work experience in Australia and Canada, as well as in Sweden where he undertook his exams for Membership of the Royal Colleges of Physicians of the United Kingdom. He returned to New Zealand in 1980 to work in a general practice on Auckland’s North Shore.
